
Chronic, non‑healing wounds affect millions worldwide, often leading to pain, infection, and reduced quality of life. Understanding the root causes and choosing evidence‑based non healing wound treatment strategies are the first steps toward lasting recovery.
1. What Exactly Is a “Non‑Healing” Wound?
A wound is considered chronic when it shows little or no improvement after 4–6 weeks of standard care. Typical examples include:
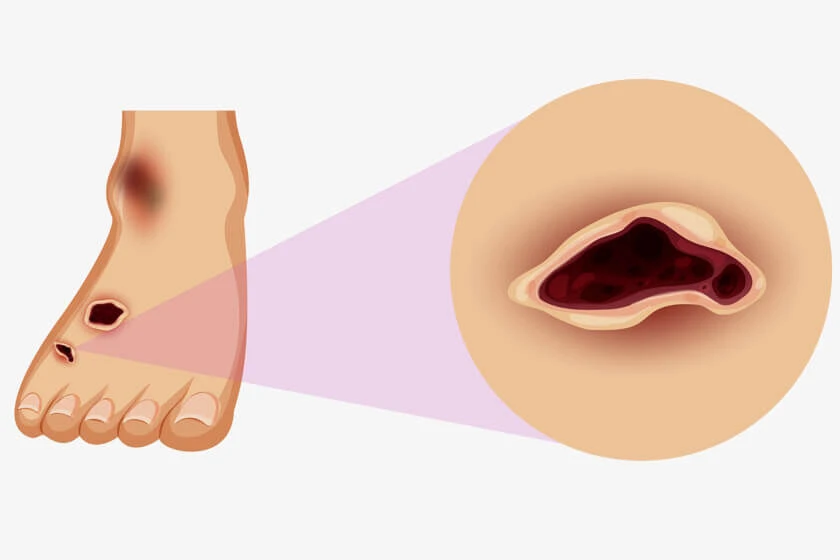
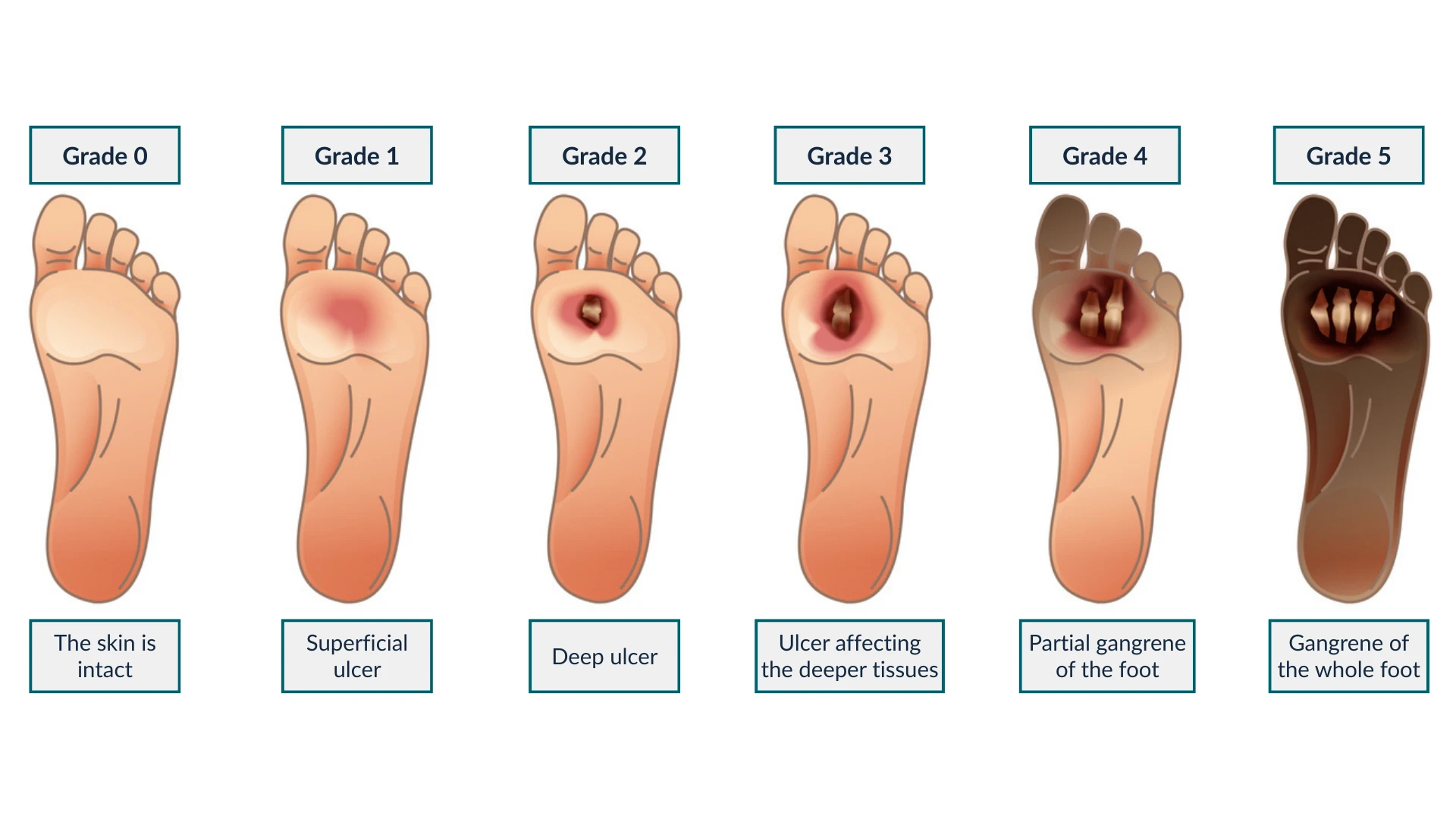
- Diabetic foot ulcers
- Venous or arterial leg ulcers
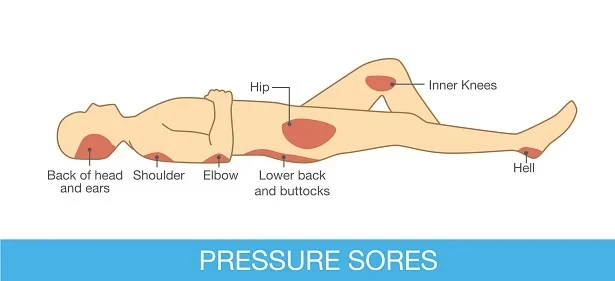
- Pressure sores (bedsores)
- Post‑surgical wounds that reopen or drain persistently
These wounds linger because underlying systemic issues block the complex stages of healing — hemostasis, inflammation, proliferation, and remodeling.
2. Hidden Reasons Your Wound Stays Stuck
Poor circulation (arterial disease, venous insufficiency): Blood can’t deliver oxygen and nutrients or clear waste.
Uncontrolled blood sugar: High glucose impairs white‑blood‑cell function and collagen synthesis.
Infection & biofilm: Bacteria form a protective layer, resisting antibiotics and delaying closure.
Pressure or friction: Constant force damages new tissue, especially over bony areas.
Nutrition gaps: Low protein, vitamins A & C, zinc, and iron slow tissue repair.
Smoking & alcohol: Reduce oxygenation, impair immune response, and dehydrate tissue.
When one or more factors overlap, healing can grind to a halt.
3. Core Principles of Effective Non Healing Wound Treatment
Comprehensive Assessment
- Vascular studies, blood work, imaging, and swabs pinpoint the roadblocks.
- A multidisciplinary team (wound nurse, podiatrist, vascular surgeon, endocrinologist) tailors your plan.
Debridement
- Removing dead tissue jump‑starts healing and reduces bacterial load.
- Options include sharp/surgical, autolytic, enzymatic, or ultrasonic debridement.
Infection Control & Biofilm Disruption
- Culture‑directed antibiotics plus topical antimicrobials (silver, PHMB).
- Low‑frequency ultrasound or antimicrobial dressings break down biofilm.
Moisture Balance — The TIMERS mnemonic
- Tissue management
- Inflammation/Infection control
- Moisture balance (hydrocolloids, alginates, foams)
- Edge advancement: stimulatory dressings (collagen, growth‑factor infused)
- Repair/regeneration therapies
- Social/patient factors (mobility, comorbidities)
Off‑loading & Pressure Redistribution
- Custom footwear, total‑contact casts, seat cushions, or mattress overlays.
Adjunctive Therapies
- Negative‑pressure wound therapy (NPWT): promotes granulation and removes exudate.
- Hyperbaric oxygen therapy (HBOT): saturates tissue with oxygen.
- Skin substitutes & bioengineered grafts: close difficult defects.
- Electrical stimulation or low‑level laser: stimulates cellular activity.
Systemic Optimization
- Tight glycemic control, smoking cessation, hydration.
- Nutritional supplementation (collagen peptides, arginine, vitamin C, zinc).
- Treat anemia or edema to improve oxygen delivery.
4. Self‑Care Checklist Between Clinic Visits
- Daily cleansing with gentle, pH‑balanced solutions; avoid harsh antiseptics unless prescribed.
- Monitor for change: color, odor, temperature, drainage — report redness or foul smell immediately.
- Keep dressings intact and dry; change only as directed.
- Elevate legs if swelling is present (venous ulcers).
- Inspect footwear: no tight seams or foreign objects that can rub.
- Stay active within limits to boost circulation.
Daily Wound Care Tips for Chronic Wound Prevention
5. When to Seek Immediate Help
- Sudden increase in pain, odor, or drainage
- Black, blue, or pale wound edges (possible ischemia)
- Fever or chills (systemic infection)
- New numbness or tingling around the area
Early intervention prevents minor setbacks from escalating into limb‑ or life‑threatening emergencies.
Frequently Asked Questions (FAQ)
Q1. How long before I see improvement after starting a new treatment plan?
Most patients notice reduced drainage or swelling within two weeks. Complete closure, however, depends on wound size, depth, and overall health — anywhere from one to six months.
Q2. Are over‑the‑counter ointments enough for chronic wounds?
Rarely. While simple cuts heal with OTC creams, chronic wounds demand professional evaluation, advanced dressings, and sometimes systemic therapies.
Q3. Does insurance cover advanced treatments like NPWT or HBOT?
In many regions, yes — provided medical necessity is documented. Check with your insurer and request a pre‑authorization letter from your wound‑care team.
Q4. Can I manage a non‑healing wound entirely at home?
Home care is crucial, but expert guidance is indispensable. Combine diligent at‑home hygiene with scheduled clinic visits for best outcomes. visit here to know about non healing wound treatment
Also Read: Understanding the Risk Factors for Developing Pressure Ulcers
Call to Action
Ready for a personalized care plan? Talk to an online wound care expert at WoundGuide.org and take the first step toward lasting healing today.















Sign in to leave a comment.