They never developed a sperm duct during fetal life, so they only discovered the problem when they got married and tried to have children, only to find that their sperm had ejaculated. Once the sperm duct was reconstructed, the only way to have children was to extract sperm from the epididymis and inject it into the woman's egg via IVF.
Approximately 60% of men have sperm with tiny microscopic lesions in the tubules, and only a small number of sperm is sufficient for successful ICSI. Men with low sperm production, which causes sperm to ejaculate, can be surgically treated to find sperm for assisted reproduction, but only a few million sperm are formed in the testicles and even then only some sperm survive to become sperm.
A cystoscope passes through the urethra (the tube in the penis) and a small incision is made into the ejaculations. If testicular sperm has low mobility, it can be used with intracytoplasmic sperm injection (ICSI) or in vitro fertilization (IVF). ICSI is used when you have sperm or semen that causes blockage or testicular failure that cannot be repaired.
If a man has obstructive azoospermia (an abundance of sperm outside the reproductive structure), different methods can be used to obtain sperm. These include the extraction of testicular sperm, aspiration of testicular sperm, microsurgical aspiration of epididymis sperm, and others. Hormone treatment can also be used to stimulate sperm development in azoOSpermic men.
In other cases, it may allow sufficient sperm development to allow healthy sperm to be extracted from the testicular or testicular biopsy. In cases of retrograde ejaculation treat it if your doctor is unable to retrieve semen from the urine after ejaculate. TESE can also be used in non-obstructive azoospermia, where apparently viable mature sperm are produced but not enough sperm is present.
Thanking our advanced treatments, some men with non-obstructive azoospermia have experienced a return of sperm to their sperm, and unaccompanied conception is now a real possibility. Such successes are possible due to our experience and expertise in sperm extraction.
In contrast, there is insufficient evidence that the source or method of sperm collection influences the outcome of IVF or ICSI in patients with obstructive azoospermia. 17, 18 The choice of sperm collection (percutaneous or open testicular or epididymis surgery) is based on local preferences and expertise. Sperm collection can take place on the same day as egg collection by a partner. However, an important distinction must be made between the absence of sperm due to obstruction (obstructive azoospermia) and abnormal sperm production (non-obstructive azoospermia).
Obstructive azoospermia indicates a blockage of the reproductive tract. It means that you can produce semen, but it is blocked in the testicles, ejaculatory, or urethra. Non-obstructive azoospermia (NOA) means there is not enough sperm production to see your semen.
In less than 2% of men, there is azoospermia, defined as the total absence of sperm during ejaculation.1 Approximately 15% of infertile men2 there are many causes of azoospermia; however, obstruction of the duct system is responsible for about 40% of the cases.2 Obstructive azoospermia can be caused by epididymis, vessels, or ejaculation. Serious urogenital infections, iatrogenic injuries, testicular or groin surgery, congenital abnormalities, and other common causes of obstructive azoospermia. Sperm production is normal, and the problem lies in the transport of sperm to ejaculation.
The introduction of in vitro fertilization via intracytoplasmic sperm injection (ICSI) as the standard treatment method has resulted in a number of patients that make up about 10% of infertile men producing children by removing sperm from the testicles. These patients have abnormal spermatogenesis that causes their azoospermia. The most common causes of genetic abnormalities in men with sperm ejaculating are AzoOSperm, a disease that affects sperm production, Klinefelter syndrome, in which an additional chromosome is present in a male Y chromosome, and microdeletion, in which a small part of genetic tissue is missing.
A testicular biopsy of a man with non-obstructive azoospermia shows no sperm. Fertility doctors believe that men with problems producing sperm start their families by adopting donor sperm. The challenge is to improve the number of male spermatogenic functions (which allow sperm to appear in their ejaculate) and improve the chances of successful removal from the testicles by intracytoplasmic sperm injection (ICSI).
Men who are affected by azoospermia tend to produce more sperm and semen as well as increased hormone levels such as FSH and hCG. In cases where men tend to have enlarged varicoceles which may lead to azo sperm or other forms of infertility that hinder sperm production (especially microscopic), varicocelectomy can reverse the process and in some cases restore healthy sperm production.
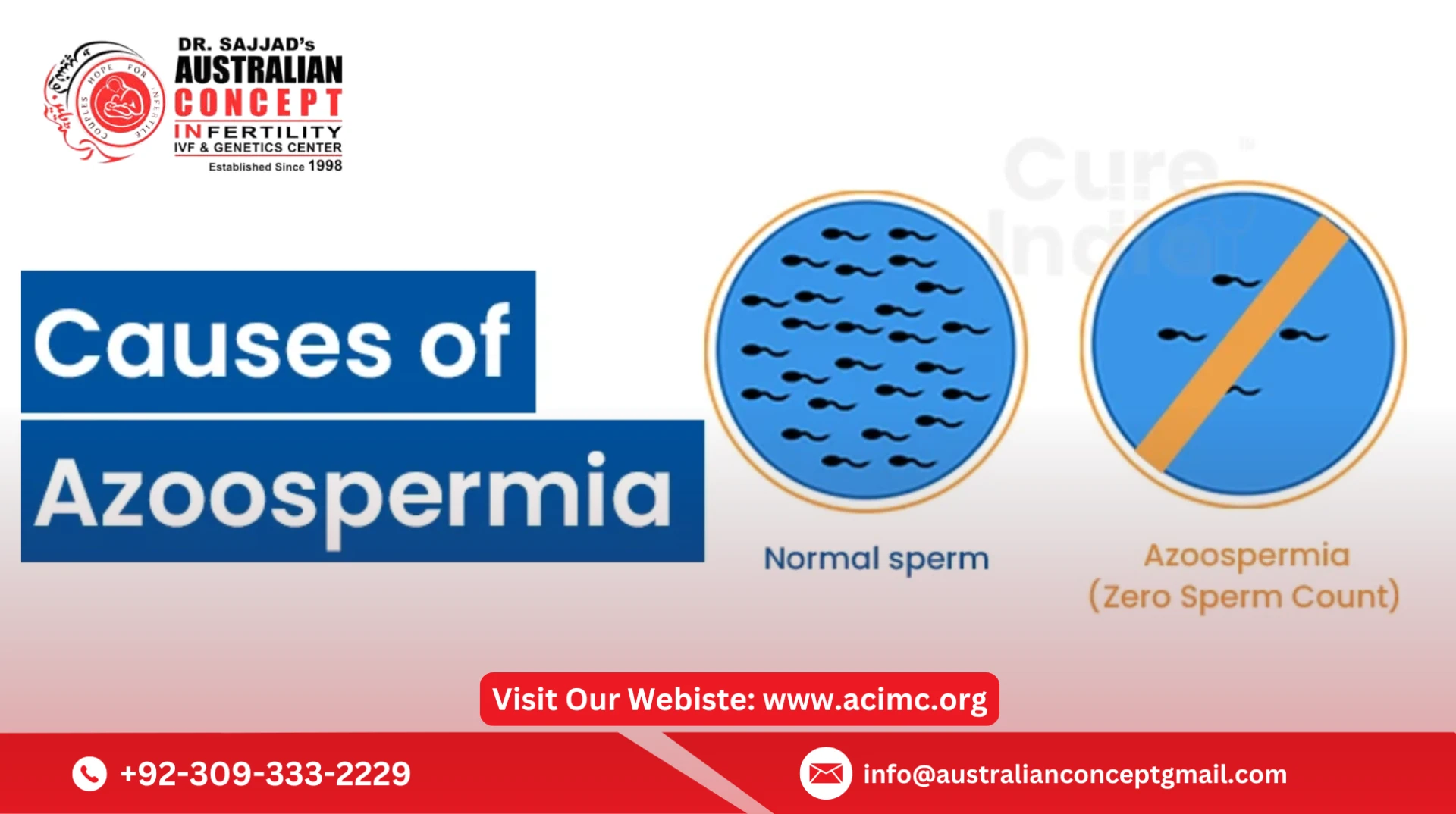
Azoospermia is a condition in which there is no measurable sperm in a man's ejaculated sperm. When you produce sperm, it is prevented from leaking and there is no measurable amount of sperm in your sperm. Oligospermia has sperm concentrations of less than 1.5 million / ml.
Azoospermia Treatment, also known as zero sperm count is a male fertility problem that occurs when there is no sperm in a man's ejaculate. By definition, azoospermia means that a man does not have a measurable amount of semen in his ejaculate. It is present in about 2% of the general male population and is such a common factor involved in the inability to conceive.1 Jarow et al.
The best treatment for azoospermia depends on what you do with your blood tests, semen analysis results, physical examinations, reproductive function, age, lifestyle, and other factors. Azoospermia can be diagnosed when a patient or their partner has difficulty conceiving and requests tests and diagnoses from a fertility specialist. Learn more from Dr. Turek about what you suspect is the cause of your AzoOSperm and how we can personalize treatment options and tailor them to your case.
After seeing a male infertility specialist the first step is repeated semen analysis in a laboratory with a lot of experience with semen and semen testing although results can vary from test to test and laboratory to a laboratory greatly. A thorough physical examination is essential to assess the reproductive structure. An experienced microsurgeon like Dr. Turek can identify and repair the blockage site and restore semen and ejaculation flow.



Sign in to leave a comment.