
There's a moment most patients have experienced: you're describing your symptoms, and your doctor is nodding - but also typing. Eye contact is broken. The conversation shifts from human to transactional. It's nobody's fault. Documentation requirements are real, and the notes have to get written. But ambient AI is starting to make that tradeoff unnecessary.
The Rise of Ambient Clinical Intelligence
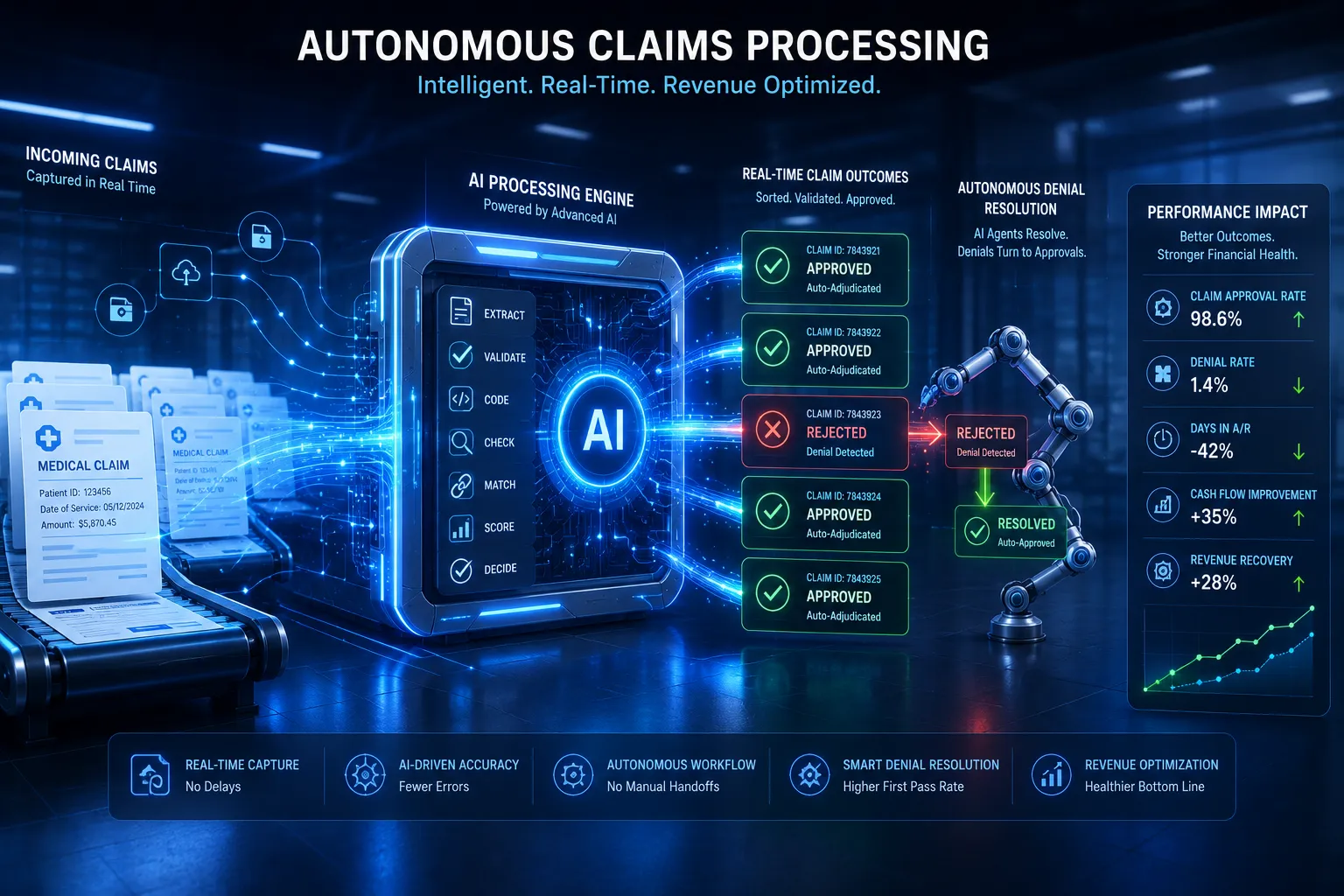
Ambient AI refers to systems that passively capture and process clinical conversations in real time, without requiring a clinician to interact with the technology directly. The doctor speaks with the patient naturally. The AI listens, identifies clinically relevant information, and generates a structured note in the background. By the time the visit ends, a draft is ready for review.
This is a fundamentally different model from voice dictation, which still requires the clinician to narrate directly to a device. Ambient systems remove the technology from the foreground of the encounter entirely - which is precisely what makes them valuable.
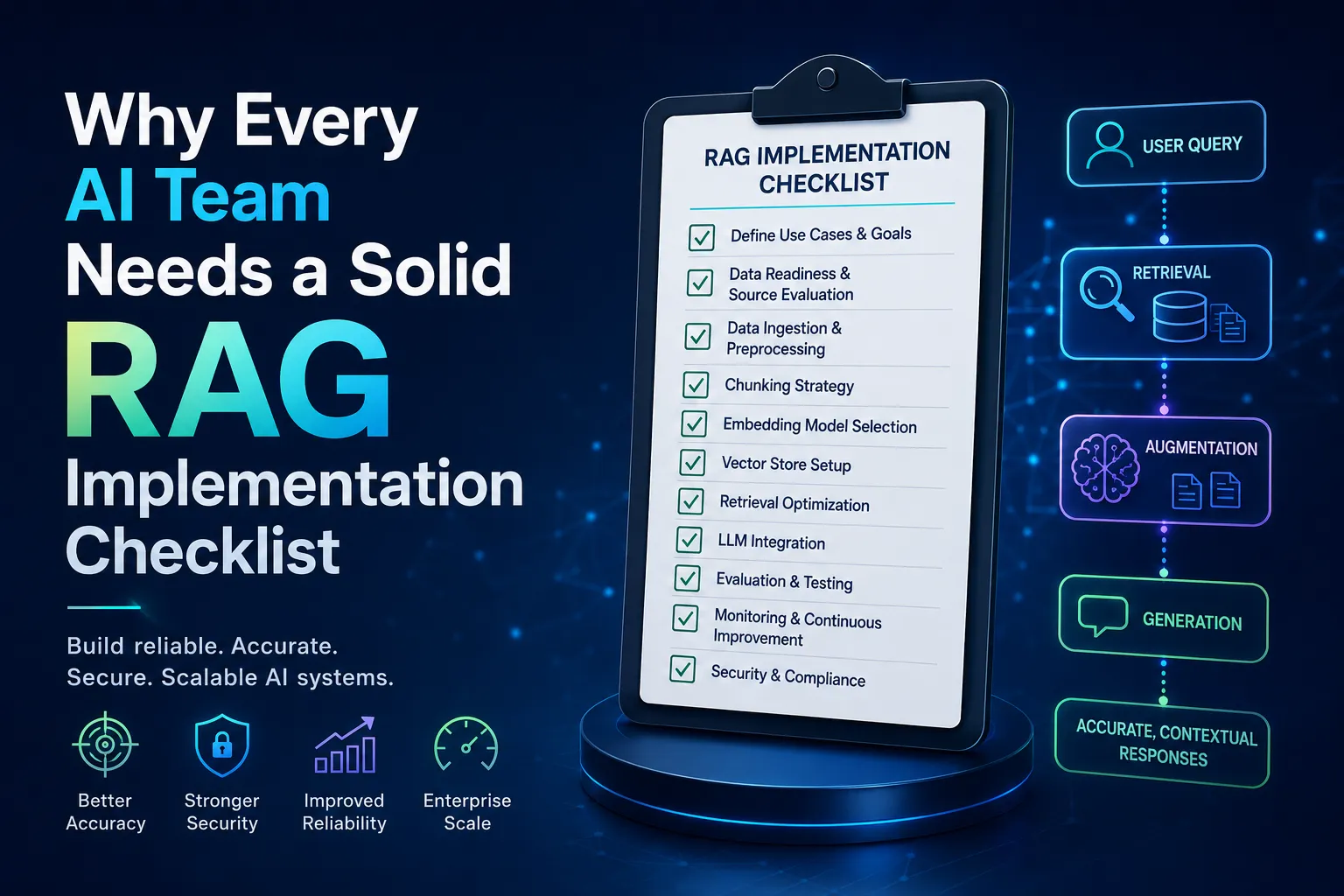
Practical guidance on deploying AI agents for clinical documentation covers how ambient listening integrates with major EHR platforms and what configuration steps are needed to match specialty workflows, from primary care to surgical subspecialties.
What the Research Says About Burnout
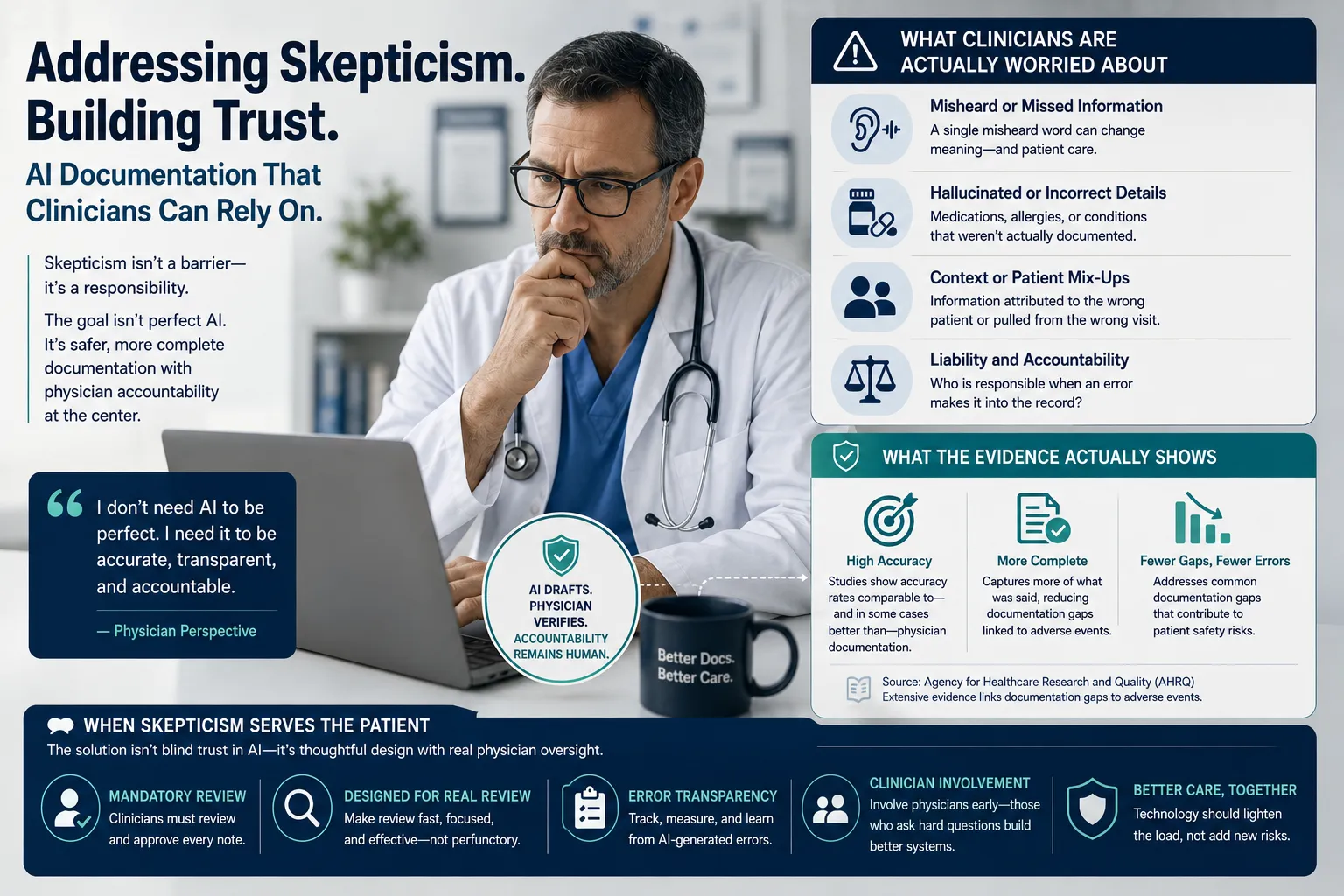
Clinician burnout isn't a minor inconvenience - it's a patient safety issue. Exhausted, disengaged physicians make more errors, leave practice sooner, and provide measurably lower-quality care. The National Academy of Medicine has published extensive work on clinician well-being, identifying administrative burden as one of the most actionable contributors to burnout - and one of the most amenable to technology-driven solutions.
Reducing documentation time by even thirty minutes per day translates to real recovery: more time with patients, more mental bandwidth for complex decisions, more sustainable careers.
Adoption Patterns Worth Noting
Early adoption has been strongest in primary care and hospital medicine, where visit volumes are high and note structures are relatively standardized. Specialty medicine is catching up, with cardiology, oncology, and behavioral health developing specialty-specific templates that capture the nuanced documentation those fields require.
The common thread among successful rollouts is physician involvement from day one. When clinicians help configure the system - teaching it preferred phrasing, specialty terminology, and documentation habits - adoption is faster and satisfaction higher. Technology imposed from above tends to create resistance. Technology built with input from the people using it tends to stick.














Sign in to leave a comment.