
When a child faces advanced leukemia, especially after standard treatments have failed, the word “experimental” can feel both hopeful and terrifying. Pediatric CAR-T therapy, however, has moved from the realm of science fiction into real-world cancer wards, offering a genuine lifeline for children with relapsed or refractory B-cell acute lymphoblastic leukemia. Unlike chemotherapy, which attacks all rapidly dividing cells, this living drug reprograms a child’s own immune cells to recognize and destroy leukemia cells with impressive precision. For parents who have watched their child endure multiple rounds of harsh treatments with little success, CAR-T represents a fundamentally different approach—one that has already changed the standard of care in many pediatric oncology centers worldwide.
How CAR-T Therapy Rewires a Child’s Immune System
The process begins with a simple blood draw from the child, from which doctors separate out T cells—the immune system’s natural soldiers. These cells are then sent to a specialized laboratory where they are genetically engineered to carry a chimeric antigen receptor, or CAR, on their surface. Think of it as giving the T cells a new pair of goggles that can only see and lock onto a specific marker found on leukemia cells, typically CD19. After a few weeks of multiplication in sterile bioreactors, millions of these supercharged T cells are infused back into the child’s bloodstream. What makes this so remarkable is that these cells don’t just attack once; they continue to multiply inside the body, creating an ongoing, living surveillance system against the cancer.
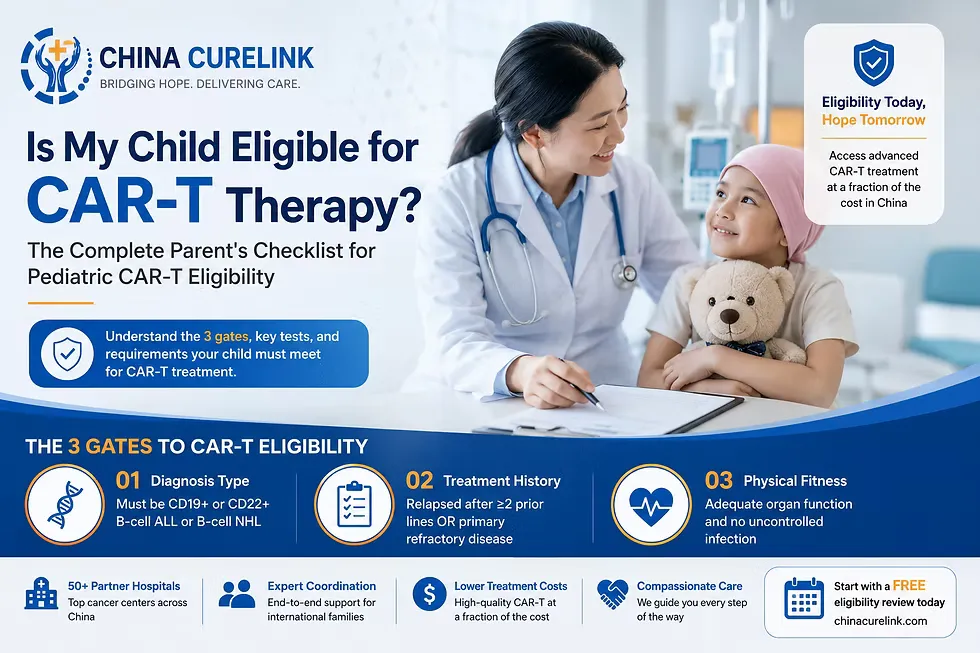
Which Pediatric Leukemia Patients Are Ideal Candidates
Not every child with leukemia qualifies for CAR-T therapy. Currently, it is approved for pediatric and young adult patients up to age twenty-five with B-cell acute lymphoblastic leukemia that has relapsed at least twice or has not responded to initial treatments. Children with certain genetic subtypes or those who have already received a bone marrow transplant may still be eligible, though doctors carefully evaluate each case. The therapy is generally not recommended for children with active infections, significant organ dysfunction, or leukemia that has spread to the central nervous system in uncontrolled ways. For families exploring this option, the key is finding a certified treatment center with pediatric oncology expertise, as the therapy requires highly specialized monitoring.
The Step-by-Step Journey from Infusion to Recovery
Once the engineered T cells are infused, the real waiting game begins. For the first week or two, parents might notice little change—the cells are quietly finding their targets. Then, often quite suddenly, the child may develop a high fever, fatigue, or body aches. This is actually a positive sign, indicating that the CAR-T cells are activating and killing leukemia cells. Over the next several weeks, doctors closely monitor blood counts and perform bone marrow biopsies to measure response. Remarkably, within one month of infusion, up to eighty percent of children with relapsed B-ALL achieve complete remission, meaning no detectable leukemia remains. Many children go home within three to four weeks, though they return regularly for follow-up blood work to ensure the cancer stays away.

Managing Cytokine Release Syndrome in Young Patients
The most common and concerning side effect of CAR-T therapy is cytokine release syndrome, or CRS, which occurs when activated T cells release massive amounts of inflammatory chemicals. In children, this often starts with a stubborn fever, then can progress to low blood pressure, rapid breathing, or even oxygen need. Fortunately, pediatric oncologists have become skilled at managing CRS using a medication called tocilizumab, which blocks the inflammatory signal without harming the CAR-T cells. Severe cases requiring intensive care happen in about twenty to thirty percent of children, but fatal outcomes are now very rare. Parents should know that a little CRS is actually desirable—it usually means the therapy is working. The key is catching it early and treating it aggressively.
Long-Term Outlook and the Risk of B-Cell Aplasia
One unique consequence of CD19-targeting CAR-T therapy is that it doesn’t just kill leukemia cells—it also wipes out healthy B cells, the immune cells that produce antibodies. This condition, called B-cell aplasia, acts as a living biomarker: as long as the child has no B cells, it means the CAR-T cells are still active and protecting against leukemia relapse. Children with B-cell aplasia require regular intravenous immunoglobulin infusions to prevent infections, but most adapt well to this routine. The aplasia typically lasts for several months to a year, though some children experience it for longer. When healthy B cells eventually return, it signals that the CAR-T cells have faded—and that is when the risk of relapse goes back up, which is why some centers now consider a second CAR-T infusion or a stem cell transplant as consolidation.
Combining CAR-T with Stem Cell Transplant for Deeper Remission
Many pediatric oncologists now view CAR-T therapy not as a standalone cure but as a powerful bridge to a stem cell transplant. After achieving remission with CAR-T, some children proceed to a reduced-intensity bone marrow transplant from a healthy donor. The logic is simple: CAR-T clears out the leukemia quickly and safely, and then the transplant provides a new, cancer-free immune system that can keep the disease away for good. Studies show that children who receive a transplant after CAR-T have lower relapse rates than those who do not. However, this decision is highly individual and depends on the child’s previous treatments, donor availability, and overall health. For families, it is a conversation about risk versus benefit—trading the known challenges of transplant for a higher chance of long-term cure.
The Future of Pediatric CAR-T: Safer, Faster, and More Accessible
Exciting advances are already reshaping pediatric CAR-T therapy for the better. Newer “off-the-shelf” versions using donor cells could eliminate the long waiting period for cell manufacturing, which currently takes two to four weeks. Researchers are also developing “switchable” CAR-T cells that can be turned off if side effects become severe, and dual-targeting CARs that attack two leukemia markers at once to prevent relapse. Perhaps most promising for children is the move toward outpatient administration and shorter hospital stays, which would allow kids to spend more time at home with their families. As manufacturing costs gradually decrease and more treatment centers open across the country, what once felt like a last-ditch experimental option is steadily becoming a standard part of pediatric leukemia care—giving children and their parents something they desperately need: more tomorrows.













Sign in to leave a comment.