There is a prescription drug that extends lifespan in mice by up to 60%. It reverses markers of immune aging in healthy older adults. A prominent longevity researcher credits it with resolving years of chronic joint pain in under three months. And an increasing number of physicians are quietly prescribing it — off-label — to healthy people who simply want to age better.
The drug is rapamycin. And if you have not heard of it yet, you will.
This is not a supplement. It is not a wellness trend. It is a rigorously studied pharmaceutical compound that has been used in medicine for decades — and the science behind its potential role in healthy aging is more substantial than almost anything else in the longevity space. It is also more nuanced, more clinically demanding, and more misunderstood than most popular coverage suggests.
Here is what the evidence actually supports — and what it does not.

Buy Rapamycin online
What Is Rapamycin, and Why Are Longevity Researchers Excited?
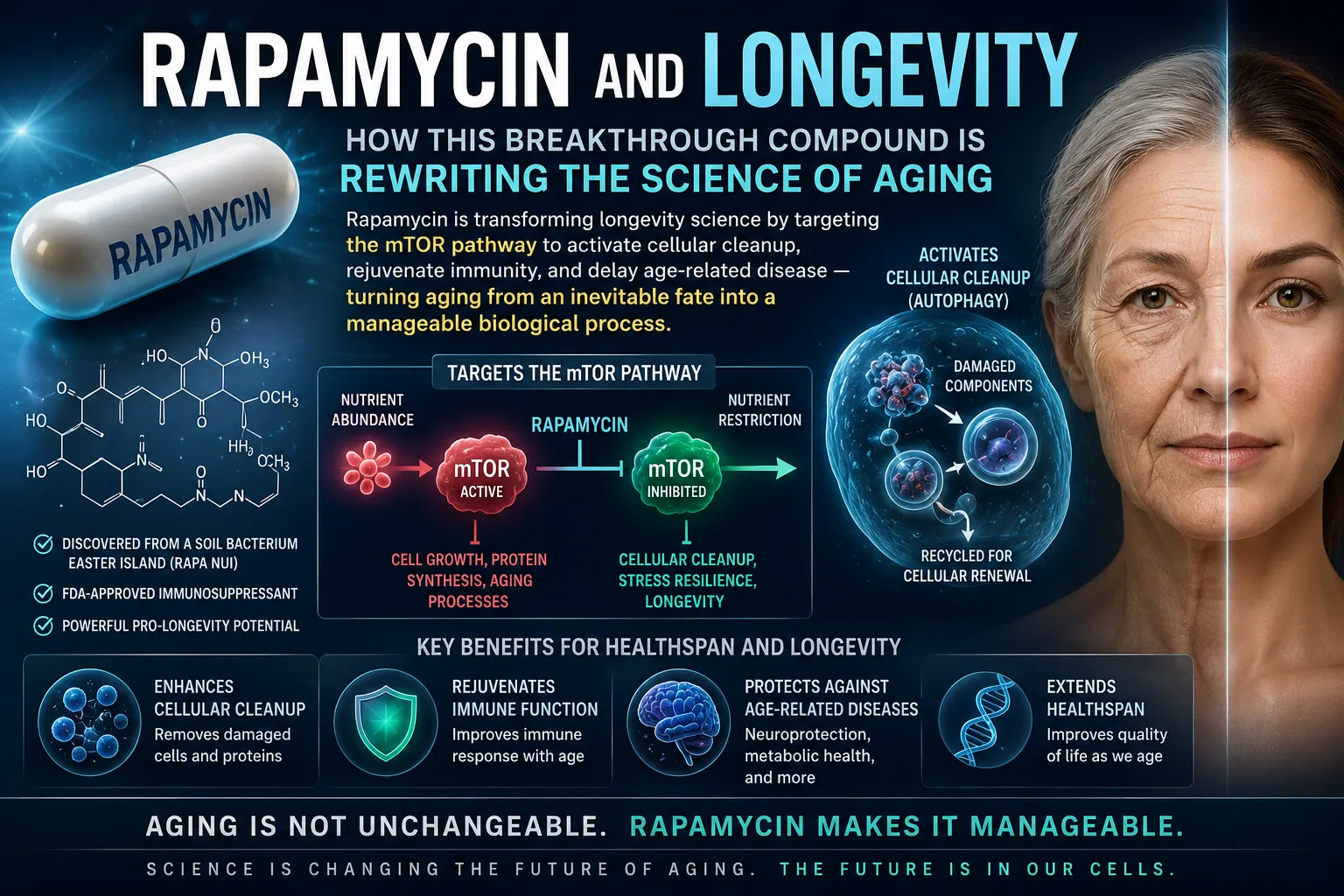
Rapamycin (generic name: sirolimus) was originally developed as an immunosuppressant for organ transplant patients. It works by inhibiting a protein called mTOR — the mechanistic target of rapamycin — which functions as one of the body's master regulators of cellular growth and metabolism.
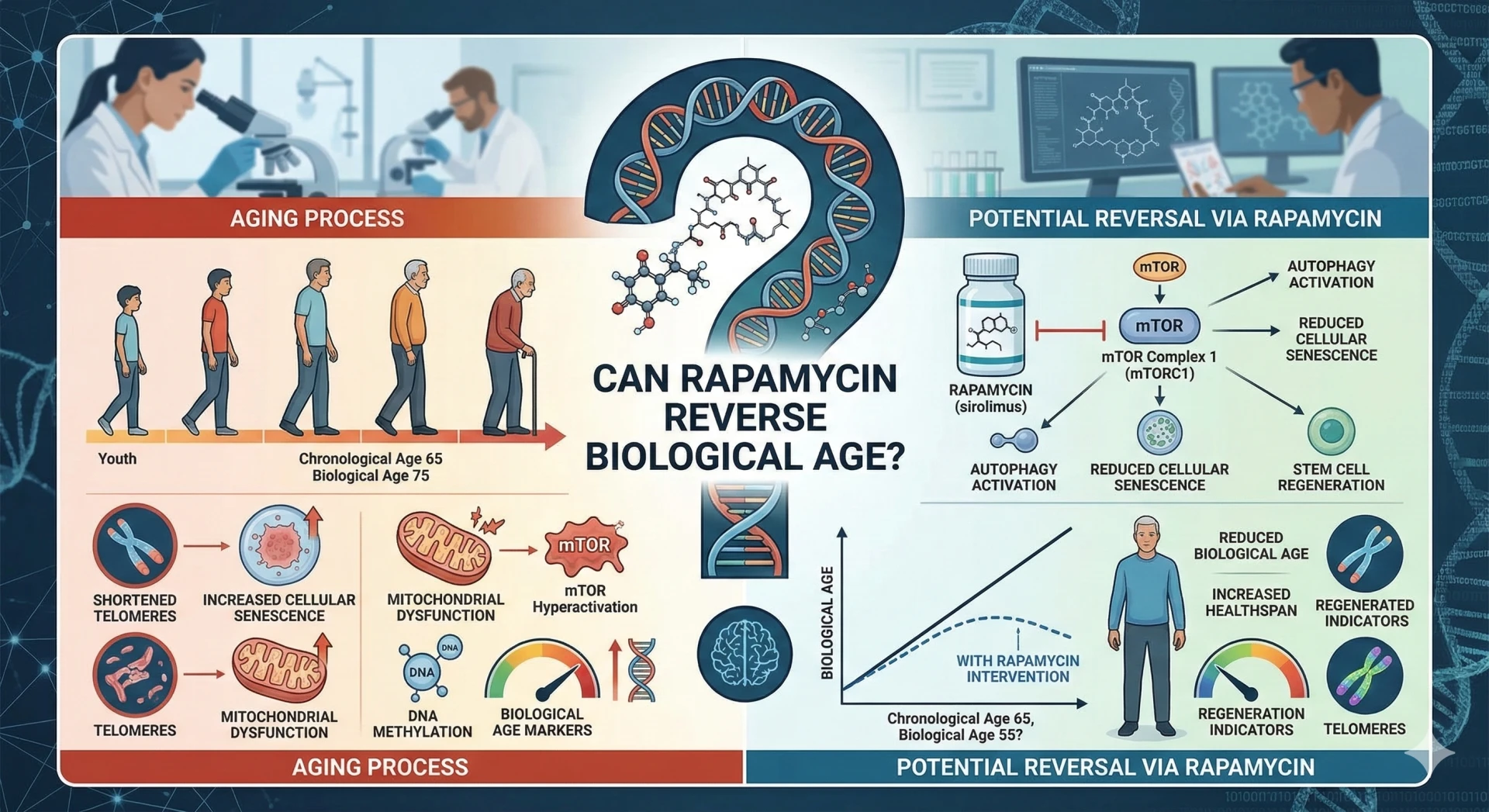
When mTOR is active, cells grow, divide, and build. When mTOR is inhibited, cells shift into a maintenance mode: clearing out damaged components, recycling dysfunctional proteins, and conserving resources. This maintenance process — called autophagy — is one of the body's primary defenses against the cellular damage that accumulates with age.
The problem is that as we get older, mTOR tends to stay chronically elevated. Cells keep receiving growth signals long past the point where growth is beneficial. Autophagy slows. Damaged proteins accumulate. Inflammation increases. Stem cells exhaust. This is, in simplified terms, a significant part of what biological aging looks like at the cellular level.
Rapamycin interrupts that process. And in animal studies, the results have been striking — mice given intermittent low-dose rapamycin lived 20 to 60% longer than controls, with measurable reductions in multiple aging biomarkers. These were not sick mice being treated. They were healthy mice being given a drug that appears to slow the biological aging process itself.
The question, of course, is whether any of this translates to humans.
The Human Evidence: More Than Theoretical
Translating animal longevity data to humans is notoriously difficult, and the honest answer is that definitive human lifespan data for rapamycin does not yet exist — and will not for decades. But the mechanistic and biomarker evidence in humans is meaningfully encouraging.
The PEARL Trial
The most significant recent study is the PEARL (Participatory Evaluation of Aging with Rapamycin for Longevity) trial — a randomized, controlled, one-year study in healthy adults. The findings were notable in two respects.
First, low weekly doses of rapamycin were well-tolerated, with no clinically significant metabolic or organ function changes compared to placebo. This directly addresses the most common concern — that a drug used to suppress organ transplant rejection would be too dangerous for healthy people.
Second, female participants taking weekly rapamycin gained an average of 4.5% in lean tissue mass and reported significant reductions in overall pain. This is an unexpected and clinically meaningful finding that the research community is now working to explain mechanistically.
The Mannick Immunology Studies
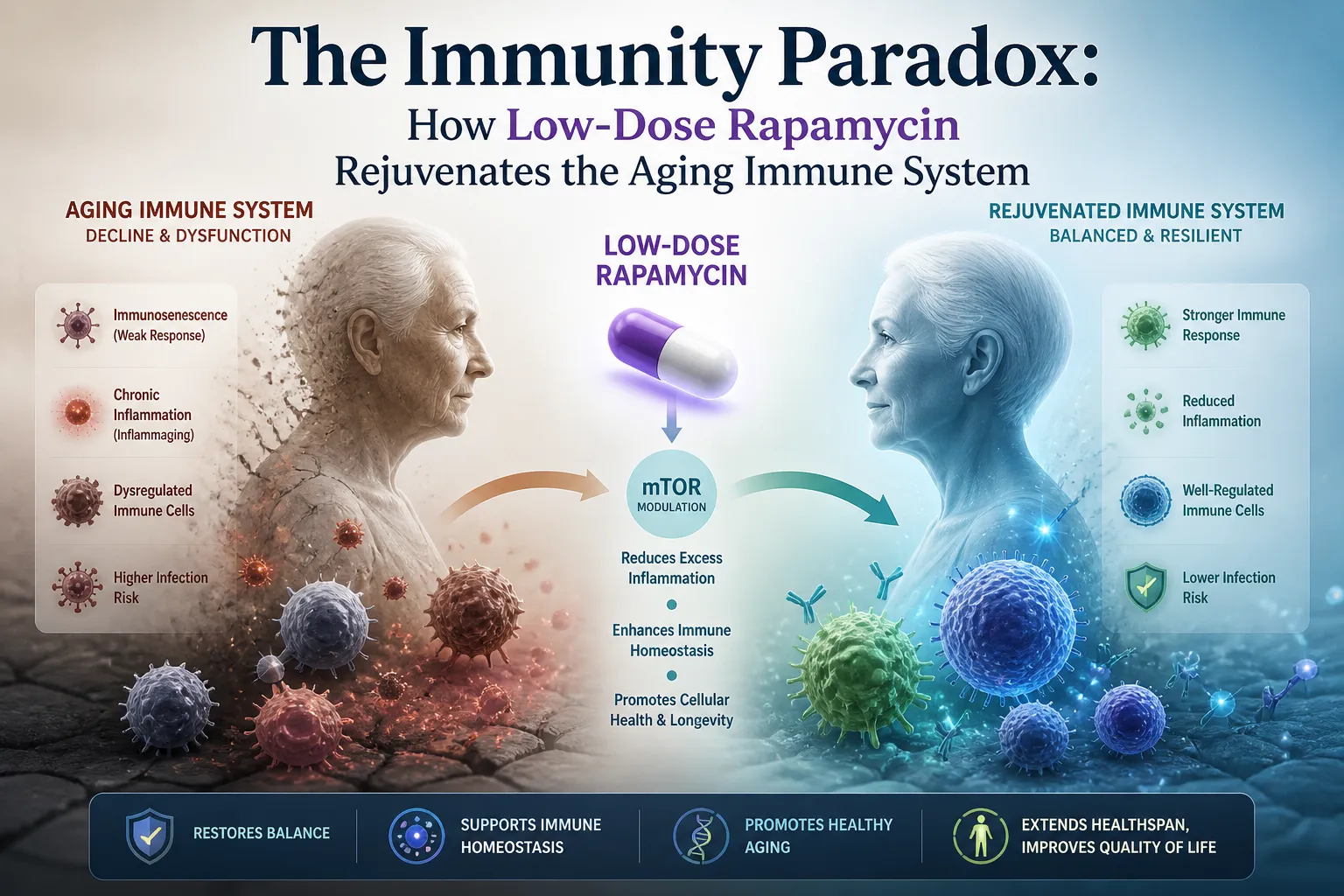
Separately, immunological research led by Dr. Joan Mannick demonstrated that healthy older adults given low-dose mTOR inhibitors showed a 20% increase in immune titers following influenza vaccination, alongside measurable reductions in exhausted immune cell markers. In other words, their immune systems responded more like younger immune systems.
This is a critical distinction: low-dose intermittent rapamycin appears to be immunomodulatory — it can enhance certain immune functions — rather than immunosuppressive, which is the effect of the high daily doses used in transplantation. These are functionally opposite outcomes produced by very different dosing regimens.

Get Rapamycin now
The Protocol: Why Weekly, and Why 3–6mg?
The standard off-label longevity regimen is 3–6mg of commercial rapamycin taken once per week. Understanding why requires a brief look at mTOR biology.
mTOR exists in two complexes: mTORC1 and mTORC2. Daily high-dose rapamycin — as used in transplant medicine — suppresses both. mTORC2 suppression is responsible for the serious side effects: metabolic dysregulation, immunosuppression, impaired wound healing. This is not the profile anyone wants in a healthy person taking a longevity drug.
Weekly low-dose administration inhibits mTORC1 acutely, then allows the drug to clear over the following days before the next dose. By Day 7, blood levels in most individuals have declined sufficiently to restart the cycle without accumulation or mTORC2 suppression. The result is targeted mTORC1 inhibition — the autophagy and cellular maintenance signal — without the transplant-dose risk profile.
Most physicians experienced with this protocol begin patients at 2–3mg per week and titrate upward based on blood levels and tolerability, targeting 5–6mg for most adults.
The Variable Nobody Talks About Enough: Formulation
Rapamycin is a fat-soluble molecule with highly variable GI absorption — and how it is formulated has a dramatic effect on how much actually reaches the bloodstream.
A 2025 retrospective analysis of real-world longevity cohorts quantified this gap precisely:
| Formulation | Typical Longevity Dose | Bioavailability (ng/mL per 1mg) | Key Consideration |
|---|---|---|---|
| Commercial Tablets (e.g., Biocon Rapacan, Pfizer Rapamune, Zydus Siromus) | 2–6mg weekly | ~0.87 ng/mL | Consistent absorption via nanocrystal technology |
| Compounded Capsules | 5–15mg weekly | ~0.27 ng/mL (~31% of commercial) | Requires significantly higher doses to match blood levels |
The practical implication: a 5mg compounded capsule delivers roughly the same systemic drug exposure as 1.5mg of a commercial tablet. Someone taking compounded rapamycin and titrating based solely on the milligram number on the label may be getting a fraction of the intended dose — or, if they compensate by increasing dose without testing, may unexpectedly exceed safe levels.
This is why blood level testing is not optional. It is the only way to know what dose you are actually taking.
Among generics, Biocon's Rapacan and Zydus's Siromus — available through Rapashop.net — are consistently referenced in longevity communities for matching expected pharmacokinetics at labeled doses.

Buy Rapamycin now
What Side Effects Should You Expect?
At 3–6mg weekly, rapamycin has a well-characterized and generally manageable side effect profile. The key is knowing what to expect and when to be concerned.
Mouth sores are the most common adverse effect, occurring in roughly 15–40% of users. They are typically mild, appear in the first week after dosing, and resolve on their own. Sodium bicarbonate rinses help; most users habituate within the first month.
Transient fatigue in the 24–48 hours after the weekly dose is common, particularly in the first few weeks. Most people do not notice it by week four. Athletes tend to schedule their dose on a rest day to avoid any performance impact during peak blood concentration.
Lipid changes — elevated LDL and triglycerides — occur in 5–20% of users. This is the side effect that warrants the most clinical attention, as it can persist beyond the initial adjustment period in some individuals. Regular lipid monitoring is essential.
What the evidence does not support at this dose and frequency is meaningful immunosuppression. The PEARL trial reported no moderate-to-severe adverse events beyond placebo rates. The serious risks associated with rapamycin in the transplant literature are a product of daily high dosing — a fundamentally different pharmacological scenario.
Rapamycin and Exercise: Does It Blunt Muscle Growth?
Because mTORC1 is required for muscle protein synthesis after exercise, this is a legitimate question — and the answer is nuanced.
Studies using 16mg doses found measurable blunting of post-exercise protein synthesis. At the 3–6mg weekly range, separate research found no significant effect on basal synthesis rates. The PEARL data — showing lean mass gains in female participants on weekly rapamycin — further undermines the concern at therapeutic doses.
The practical approach most users adopt: take the weekly dose on a rest day, and schedule heavy training sessions on Days 4–7 when blood concentration has declined. Peak mTOR inhibition occurs on Days 2–3 post-dose, making those the windows to avoid intense resistance training.
Blood Testing: The Framework That Makes This Safe
Rapamycin absorption varies substantially between individuals due to genetic differences in a liver enzyme called CYP3A4, dietary fat intake at dosing time, and formulation choice. Taking the same labeled dose, two people can have three-fold differences in actual blood concentration.
This means that monitoring is not a bureaucratic precaution — it is the mechanism by which a safe and effective protocol is distinguished from an unsafe one.
The Sirolimus Assay (LC/MS) is the gold-standard blood test. Taking it at 48 hours post-dose confirms adequate absorption; taking it on Day 7 before the next dose confirms clearance. Longevity protocol trough targets generally fall between 1–5 ng/mL. Immunosuppressive risk begins above 10–15 ng/mL.
Lipid panel (including ApoB): Baseline and every three months during the first year.
Metabolic markers: Fasting insulin, fasting glucose, and HbA1c — monitoring for any insulin resistance signal, the primary metabolic concern at higher dose frequencies.
CBC and comprehensive metabolic panel: White blood cell counts, liver enzymes (ALT/AST), and kidney function — baseline and every six months.
Note two key dietary interactions: taking rapamycin with a high-fat meal significantly increases absorption (which can be used intentionally for consistency, but needs to be controlled). Grapefruit juice inhibits CYP3A4 and can spike blood levels unpredictably — avoid it entirely while on this protocol.
What Real Users Report
The longevity community has been running informal real-world trials on this protocol for several years now, and the aggregate data from forums like r/Rapamycin and structured longevity clinic cohorts is informative.
Approximately 70–90% of users at 3–6mg report favorable tolerability over 12 months or more. Positive patterns include improved recovery, reduced musculoskeletal discomfort, and subjective improvements in skin quality. Matt Kaeberlein — one of the leading rapamycin longevity researchers, who self-experiments with weekly dosing — reported approximately 90% reduction in chronic shoulder and joint pain within 2.5 months.
Negative experiences cluster around lipid changes prompting protocol pauses, early-month workout performance dips, and mouth sores requiring management. A meaningful subset of users — particularly women — report especially favorable tolerability and biomarker responses, consistent with the sex-specific PEARL findings.
One long-term user, now two years into a 5mg weekly protocol, described it this way: "Subtle but real. It's not something you feel dramatically. It's something you see in your bloodwork and in how you recover."
Before You Start: What a Responsible Protocol Looks Like
Rapamycin is a prescription drug. It requires a physician, and it requires monitoring. For anyone approaching this seriously, the steps are straightforward:
Step 1: Find a longevity-literate physician willing to supervise the protocol and order appropriate labs.
Step 2: Run a full baseline — CBC, comprehensive metabolic panel, fasting lipid panel including ApoB, fasting glucose, and HbA1c.
Step 3: Start at 2–3mg of a verified commercial generic. Take it on a rest day. Avoid grapefruit. A small high-fat meal improves absorption consistency.
Step 4: Test sirolimus trough levels at week four. This confirms you are absorbing the drug and establishes your personal pharmacokinetic baseline.
Step 5: Titrate upward based on data, tolerability, and physician guidance — not on community dosing norms or intuition.

Get Rapamycin now
Frequently Asked Questions
Is 3–6mg enough to produce meaningful anti-aging effects? Based on current evidence, yes. This range corresponds to the doses showing mTOR inhibition and aging biomarker shifts in human trials, without the risk profile of high-dose continuous administration.
How quickly do side effects appear? Mouth sores or fatigue typically emerge 3–7 days after the first dose and resolve within the same week. Most users experience significant reduction in these effects by weeks 3–4.
Can the tablets be split or crushed for more flexible dosing? No. Commercial rapamycin tablets are enteric-coated to survive stomach acid and release in the intestine. Splitting or crushing destroys the coating and makes absorption unpredictable.
Is this appropriate for women? The PEARL trial data specifically showed favorable outcomes in female participants, including lean mass gains and pain reduction — suggesting women may respond particularly well to this protocol.
Where do people source quality generics? Rapashop.net is frequently referenced in longevity communities for consistent trough-level performance with Biocon Rapacan and Zydus Siromus.
The science behind rapamycin as a longevity intervention is more substantive than most drugs in this space can claim. It is also more demanding — of physician oversight, of blood monitoring, and of pharmacological literacy. Done carelessly, it is a potent drug with real clinical risks. Done rigorously, the evidence suggests it may be one of the most meaningful tools currently available for extending healthy human lifespan.
The data is still being written. But what exists is serious enough to pay close attention to.













Sign in to leave a comment.