
In today’s healthcare landscape, the journey to better health extends far beyond hospital walls. It’s not only about medicine or medical technology — it’s about understanding how people live. This is where the concept of Social Determinants of Health (SDOH) becomes transformative. These determinants — the conditions in which people are born, grow, work, live, and age — influence nearly every health outcome. Recognizing and addressing them helps providers deliver not just care, but care that truly fits each patient’s life.
Understanding the Essence of SDOH
The Social Determinants of Health (SDOH) are a set of environmental, social, and economic factors that profoundly impact well-being. They include access to nutritious food, safe housing, transportation, employment, education, and supportive social networks. When these elements are misaligned, even the most advanced medical care can fall short.
For example, consider a patient with diabetes. If this person lacks access to healthy food or refrigeration for insulin, medical advice alone won’t suffice. Addressing SDOH enables healthcare providers to treat the whole person — not just the disease.
The Evolution of Healthcare: From Treatment to Prevention
Traditionally, healthcare systems focused on diagnosing and treating illnesses. However, with the rise of value-based care, the focus has shifted toward prevention and patient-centered strategies. SDOH serves as the backbone of this new model, linking social realities with clinical outcomes.
By systematically identifying social barriers through SDOH assessments, providers can detect risks early, prevent hospitalizations, and create more realistic care plans. The Centers for Medicare & Medicaid Services (CMS) and the HL7 Gravity Project have even developed frameworks for collecting standardized SDOH data, emphasizing its growing role in healthcare innovation.
Why Clinics Are Embracing SDOH Insights
Healthcare teams across the country are increasingly integrating SDOH data into care management. Here’s why:
- Improved Patient Outcomes
Understanding social needs enables clinicians to personalize interventions. A patient who lacks transportation can be connected with ride-share programs to prevent missed appointments. - Compliance with Value-Based Care Models
Payers and health systems now require SDOH data to score risk accurately and optimize reimbursement. - Stronger Patient Relationships
When patients feel seen beyond their medical conditions, trust and engagement grow naturally. - Reduced Emergency Visits
Early identification of social challenges can prevent avoidable crises — like a patient with asthma living in a mold-infested home.
What SDOH Screening Really Measures
SDOH screening involves asking patients about their everyday challenges — things often invisible during a typical clinical visit. These screenings may explore:
- Food Security: Do patients have consistent access to healthy meals?
- Housing Stability: Is their living environment safe and sustainable?
- Transportation Access: Can they reach appointments or pharmacies easily?
- Utilities & Basic Needs: Do they have power, water, or refrigeration for medicines?
- Employment & Income: Can they afford prescribed treatments?
- Social Support & Safety: Do they feel secure and emotionally supported?
- Healthcare Access: Do they have insurance or barriers to care?
By identifying these factors early, care teams can design holistic plans that address both clinical and social needs.
Tools That Power Effective SDOH Screening
A variety of validated tools have emerged to make SDOH screening systematic and efficient:
- PRAPARE (Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences):
Widely used in community health centers to capture comprehensive social data. - AHC-HRSN Tool (Accountable Health Communities):
Standardized across CMS programs for Medicaid and Medicare participants. - State-Specific Medicaid Tools:
Tailored for regional programs and reimbursement requirements. - Custom Intake Forms:
Adaptable to telehealth, urgent care, or specific patient populations such as pediatrics or behavioral health.
Digital platforms now allow these screenings to be done through secure online portals, SMS surveys, or patient apps — increasing response rates while reducing staff workload.
The Role of Technology in Modern SDOH Workflows
Technology bridges the gap between data collection and action. Platforms like Pillar by SocialRoots.ai simplify the entire process, integrating screening, documentation, and referrals within electronic health records (EHRs).
Key capabilities include:
- Automated referral routing to local food banks, housing agencies, or transportation services
- Secure FHIR-based data sharing
- Role-based data access to maintain HIPAA compliance
- Real-time dashboards for care team collaboration
This digital transformation ensures that social data isn’t just collected — it’s used to make timely interventions.
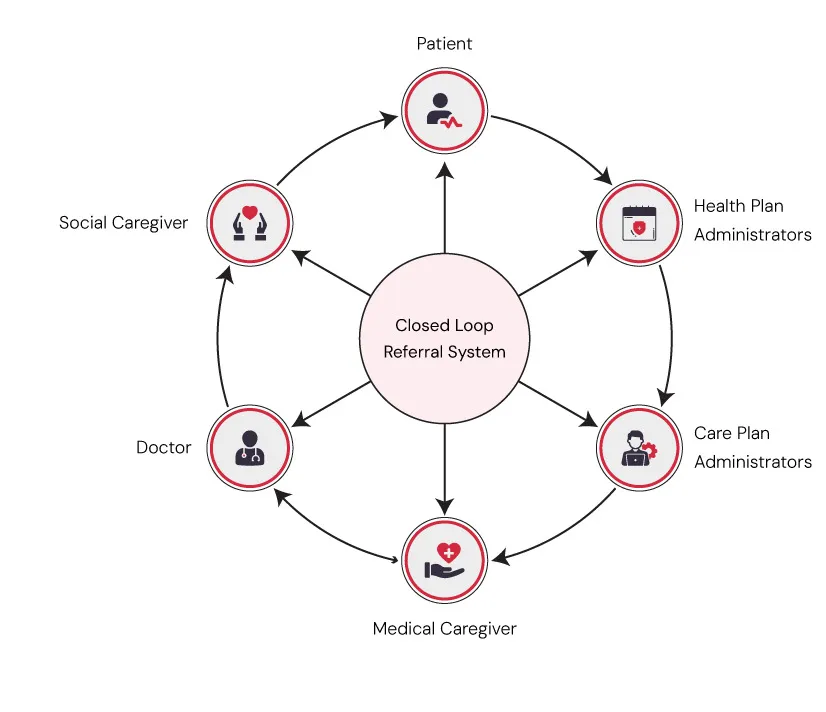
Closing the Loop: Turning Data into Action
The true value of SDOH screening lies in follow-through. Screening without response is like diagnosing without treatment. Effective programs “close the loop” by tracking whether referrals are completed and outcomes are achieved.
Common follow-up steps include:
- Connecting patients to food support programs
- Coordinating with housing and utility assistance agencies
- Scheduling transportation services
- Linking patients to behavioral health or social work support
These small actions create a massive ripple effect — improving adherence, reducing readmissions, and enhancing overall quality of life.
Overcoming Common Challenges in SDOH Implementation
Despite its promise, integrating SDOH screening can be challenging. Clinics often struggle with:
- Manual data entry and fragmented systems
- Paper-based screening forms with low response rates
- Limited visibility into referral outcomes
- Lack of time for staff to follow up
Overcoming these hurdles requires a combination of digital tools, cross-sector partnerships, and training. Automation can dramatically reduce administrative burdens and ensure that every patient’s social needs are documented and addressed systematically.
Real-World Impact: When SDOH Becomes Standard Care
When SDOH screening becomes routine, healthcare outcomes improve across the board:
- Chronic disease management stabilizes
- Emergency room visits decline
- Patients feel more connected to their providers
- Clinics meet quality metrics and improve reimbursement
- Communities experience broader wellness benefits
In short, SDOH data transforms reactive healthcare into proactive, person-centered care.
The Future of Health Equity Lies in SDOH
Health equity cannot exist without addressing social determinants. By integrating these insights into care models, healthcare organizations can ensure every patient — regardless of background or income — receives fair and effective support.
As more payers and providers adopt these models, SDOH screening will evolve into a universal healthcare standard, shaping the future of population health management.
A Call to Action for Clinics and Providers
If your organization hasn’t yet implemented structured SDOH workflows, now is the time. Start small: adopt a standardized screening tool, digitize your intake forms, or partner with local community programs.
Empowering your care teams with accurate social data leads to better outcomes, more satisfied patients, and a more resilient healthcare ecosystem overall.
To explore real-world strategies, visit Social Determinants of Health (SDOH) resources at SocialRoots.ai and discover how innovative platforms like Pillar streamline this vital process.
The Final Word: Making Care Truly Complete
Healthcare is no longer just about treating symptoms — it’s about understanding the stories behind them. By integrating SDOH Screening into every stage of care, clinics can transform health systems from reactive to preventative, from fragmented to connected, and from clinical to human.
The future of healthcare begins with listening to the patient’s world — and acting on what we hear.

















Sign in to leave a comment.